

Hi, I am Mandy Irby and I’m here with Maggie Runyan and Paula Richards.  And we are all three co-founders of the trauma informed birth nurse program, and we’re all bedside nurses in addition to other specialties, such as nurse educators, healthcare consultants, AWHONN educator, parent educators, entrepreneurs, lactation counselor, and nonprofit founders.
And we are all three co-founders of the trauma informed birth nurse program, and we’re all bedside nurses in addition to other specialties, such as nurse educators, healthcare consultants, AWHONN educator, parent educators, entrepreneurs, lactation counselor, and nonprofit founders.
As nurses, it’s not our job to diagnose, to understand everything about someone. But so often we have that pressure put on us. When we are over here in this helper nurse role, we either have been kind of pinpointed as the handmaiden, or the hero of the situation.
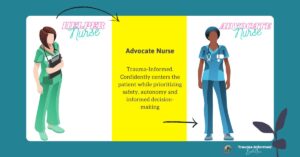
And, you know, both of those really take us away from truly connecting with our patients. Trauma informed care is a way for us to more confidently – step into that advocate nurse role, where we are centering our patients, prioritizing their safety, autonomy, and ensuring informed decision making. Of course these are our everyday goals. They can feel impossible when the priority is on centering the facility’s bottom line, however.
But so many times there are myths misconceptions about person-centered care and about trauma informed care, and we want to break some of those down for you.
So first is our awareness around it. Often we have been taught that trauma informed care is only for those people over there. Right? We think of folks who’ve experienced sexual assault, medical trauma like motor vehicle accident or hemorrhage, those who are in an intimate partner violence relationship, someone who’s lost their partner, or has lost a pregnancy, or anyone who discloses specifically that they have a history of trauma. They are the folks who need this type of specialized care.
However, the reality is, it’s so much easier than that. Trauma informed care is for every person, for every reason, for every birth.  When we get away from that feeling of needing to diagnose and to dissect someone’s story and instead shift our standard of care to being one of trauma-informed care for each person, it’s actually so much easier for us.?
When we get away from that feeling of needing to diagnose and to dissect someone’s story and instead shift our standard of care to being one of trauma-informed care for each person, it’s actually so much easier for us.?


Click on the video below and share with a nurse colleague or educator 

