Rather than their decisions being dictated by what makes providers comfortable, birth care that recognizes trauma puts the patient at the helm. Patients are more satisfied when they get to dictate their care, and HCAHPS results increase.
This cutting-edge training puts hospitals and systems ahead of the curve, while others still use outdated methods that traumatize patients and put more pressure on providers. And there’s a special new designation for hospitals that prioritize birthing care. Let’s talk about it.
The “Birthing Friendly” Designation
In December 2021, the White House issued a national call to action to reduce maternal mortality and morbidity rates in the United States. The US has long had some of the highest maternal illness and death rates among high-income nations. Among minority populations, these rates are even higher due to systemic racism and discrimination. In 2020, the rate of death for Black birthers was found to be three times the rate for white birthers, and had risen from 2019.[6]
In 2023, the Department of Health and Human Services (DHHS) will establish a separate, publicly-reported hospital designation for hospitals prioritizing maternal health outcomes. The Centers for Medicare & Medicaid Services (CMS) have released a guidance memo that encourages hospitals to implement the following:[7]
- Evidence-based best practices for managing obstetric emergencies
- Interventions to address factors that contribute to maternal health disparities
To support these changes, the Biden-Harris administration plans to establish a “Birthing-Friendly” designation through the 2023 President’s Budget. This public-facing hospital designation reflects investments in the quality and safety of maternal care. The first-of-its-kind quality designation will set hospitals apart for families looking for birthing care.
This is good news for birthing families, who will soon have more ways to evaluate a hospital or birthing unit before going in for care. But it also means hospitals that don’t pursue safer, higher-quality birth care may soon find fewer families coming to them. The good news is trauma informed birthing care training checks off both boxes.
Trauma informed care training helps care teams communicate better with patients and each other in emergencies. It also helps providers establish a baseline of trust. And many of the factors that contribute to health disparities are associated with implicit bias.[8] By helping clinicians understand differences in care and the trauma they can cause, our training improves marginalized maternal care.
Trauma informed birth training also fits into existing safety bundles. Let’s talk about which bundled care measures can improve after implementing this training.
Measurable Improvements to AIM Patient Safety Bundles
Bundled care programs help hospitals improve care processes and outcomes. The Alliance for Innovation on Maternal Health (AIM) tracks adherence to standardized care bundles. Some specific bundles even have state-tracked metrics, allowing public health authorities to track more complex outcomes, such as maternal mortality.
Our program fits within several AIM safety bundles and increases adherence to specific patient safety measures. Our program helps hospitals adhere to every maternal care bundle because this education helps units provide respectful, safe care. Here are a few specific ways our program helps units and hospitals consistently implement bundled care:
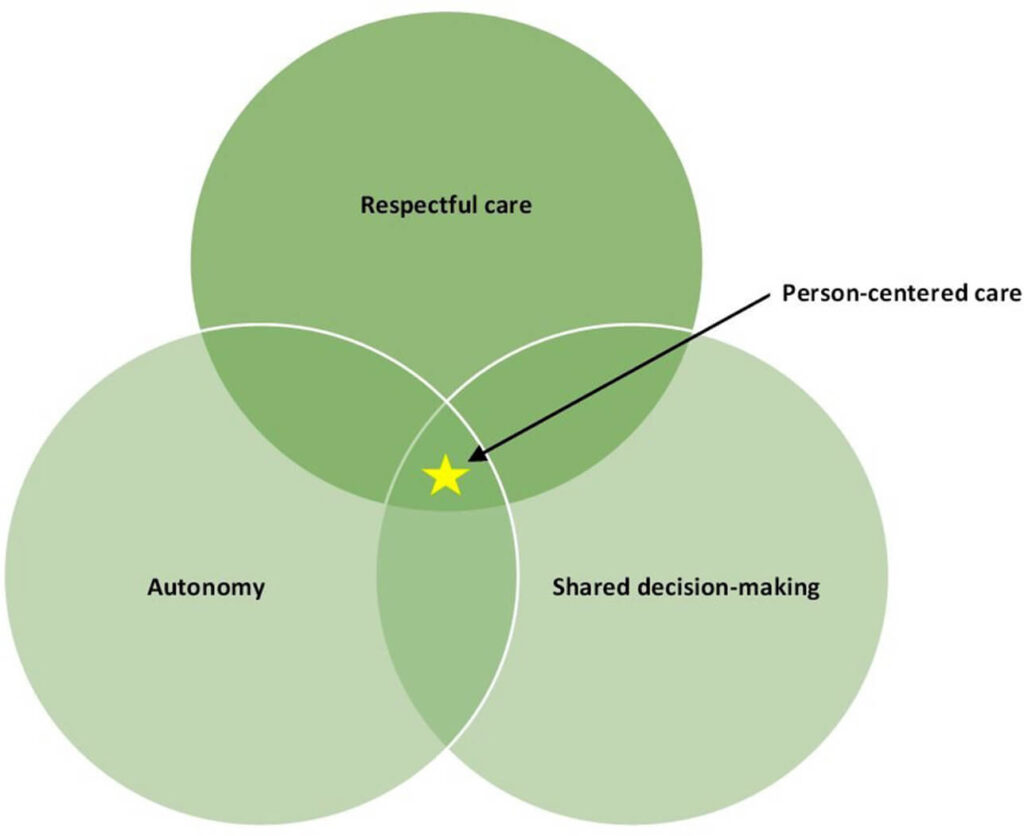
- Every AIM safety bundle requires respectful, equitable, and supportive care. This requires every team member to communicate openly, transparently, and empathetically with patients. Peripartum persons must be key decision-makers in their care. Their unique values and goals must be reflected in the shared goals of the care team. In addition, patients have the right to respectful refusal. All of these requirements are met within trauma informed care training.
- The AIM obstetric hemorrhage bundle requires additional staff support for patients who refuse blood products. It also requires further review of the root causes of disparities in hemorrhage care. Pre-birth education ensures patients understand the signs and risks of birth. Trauma-informed training helps clinicians understand and respect patients’ decisions for blood treatments and encourages more thorough education to address these bundle goals.[9]
- The AIM cesarean reduction bundle requires units to build a culture that “values, promotes, and supports spontaneous onset and progress of labor and vaginal birth.” Under trauma informed care, patients aren’t pressured to induce or undergo a cesarean without indication, which is an immediate requirement of this safety bundle. We help units maximize the likelihood of safe vaginal birth while using shared decision-making processes to reduce unnecessary and unwanted c-sections.[10]
Our training helps units adhere to AIM safety bundles in more ways than one. That’s because our one-stop unit programs help teams develop as a whole. To improve whole-patient safety, you have to educate the whole unit. But what impact does this program have on costs related to adverse safety events? Here’s how trauma informed training helps units save on patient safety costs.

Trauma Informed Training Decreases Patient Safety Costs
Adverse safety events in the hospital are linked to greater care costs and higher spending during the acute care period and after discharge.[11] Trauma informed training helps reduce the costs associated with adverse safety events in the OB setting. It also decreases the psychological trauma that birthing events can cause for patients and families.
Birth can be risky, and some of these risks are impossible to control. A study published in 2022 found that the most common triggers for safety events in birthing care weren’t maternal health but problems within health systems. Researchers noted that better training in team communication could reduce these health events and hospital spending.[12]
For example, cesarean delivery rates have increased substantially in the last few decades. Yet we know that C-sections are associated with worse safety and efficacy for birthers and infants.[13] C-sections are associated with tripled rates of severe maternal morbidities, compared to vaginal deliveries.[14] Education for parents and clinicians has strongly shown to decrease these rates.[15]
For example, our training helped Iowa hospitals decrease safety-related costs by preventing unnecessary c-sections. In 2020, their cesarean delivery rates were projected to rise by 2%. But after we trained 200 of their staff in a live, virtual workshop, their cesarean delivery rates decreased by 2%.[16]
From a risk management perspective, harm reduction training is a win-win. Administrators can decrease safety events and the associated costs, while clinicians feel safer under the trauma informed care model. Let’s talk about the impacts of trauma informed birth training on patient outcomes.
Trauma Informed Care Increases Patient Safety
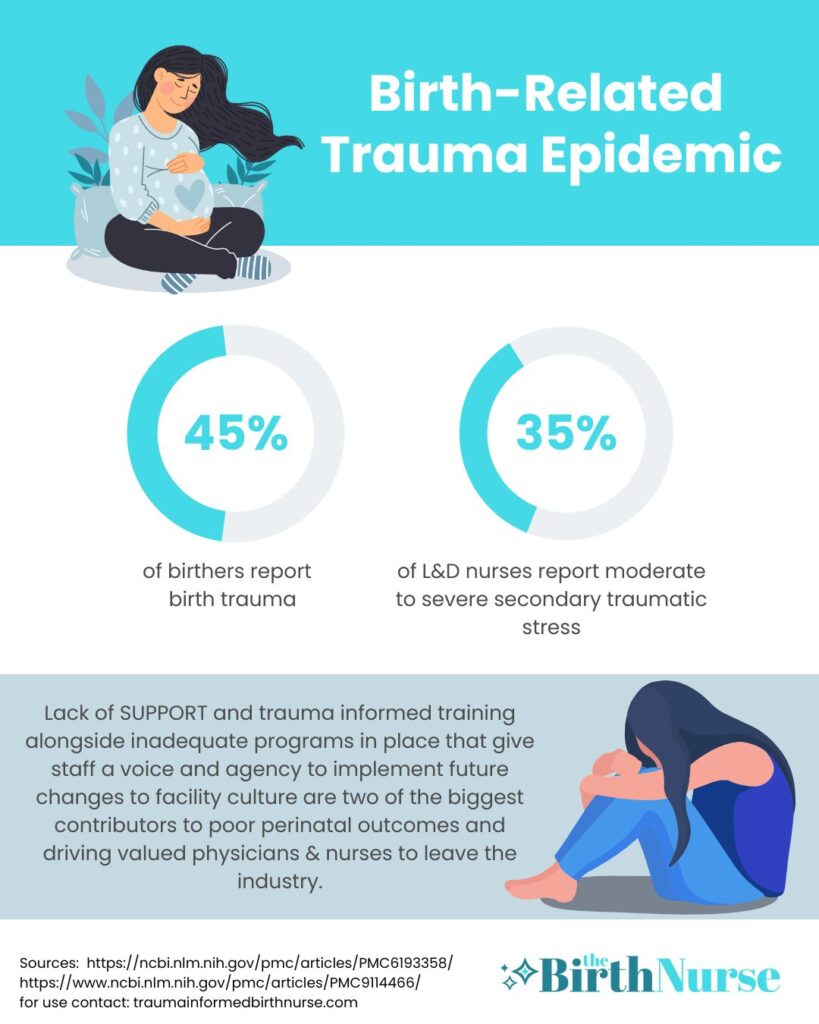
Traumatic experiences can be mitigated with education, support, culture shifts, and proper care. Yet they happen more often than they should. Nearly half of first-time mothers experience trauma during their birthing experience. Rates of PTSD after birth trauma are up to 18.5% in high-risk groups.[17],[18]
To make matters worse, previous trauma makes women more vulnerable to traumatic birthing experiences. Sexual abuse survivors are more likely to be re-traumatized during birth. Women with prior mental health diagnoses and poor relationships with their providers are also at higher risk.[19],[20]
When we think about the consequences of psychological trauma, PTSD is the first diagnosis that comes to mind. Of pregnant, birthing, and postpartum people, 9% have a diagnosis of PTSD.[21] But this isn’t the only downstream effect for people with traumatic childbirth experiences. Here’s a list of other associated effects of birthing trauma:
- Risk for problems with breastfeeding[22]
- Increased risk for postpartum depression[23]
- Increased risk for psychosis and anxiety[24]
- Increased risk for emergency cesarean delivery[25]
- Increased risk for postpartum hemorrhage
Traumatic experiences during birth cause harm to patients in more ways than one. This quote by birthing trauma researchers puts this point beautifully: